EKG Foundations
How to read an ECG from the ground up: the waves and intervals, the grid they sit on, and a step-by-step method for naming any rhythm.
The electrocardiogram (ECG, or EKG) is a recording of the heart's electrical activity, captured at the surface of the body and traced onto calibrated paper. With every heartbeat, an electrical impulse travels through the heart in a fixed sequence; electrodes placed on the skin detect that impulse and plot it as a series of waves. It is one of the most valuable tests in medicine. Quick, painless, and inexpensive, it can still reveal the heart's rate, rhythm, and conduction, along with signs of ischemia, injury, and many other conditions.
To the untrained eye an ECG looks complicated, but it is built from only a handful of waves, and they appear in the same order with every beat. Each one corresponds to a specific electrical event in the heart, with a characteristic shape and a defined normal range. Once you understand what produces each wave and how to measure it, interpretation becomes a systematic, repeatable process rather than guesswork. This page builds those fundamentals from the ground up: the conduction system, the waves and intervals, the grid they are drawn on, and a step-by-step method for reading any rhythm.
The conduction system
A heartbeat is an electrical wave that sweeps through the heart in a fixed order. The ECG is simply a recording of that wave from the body surface.
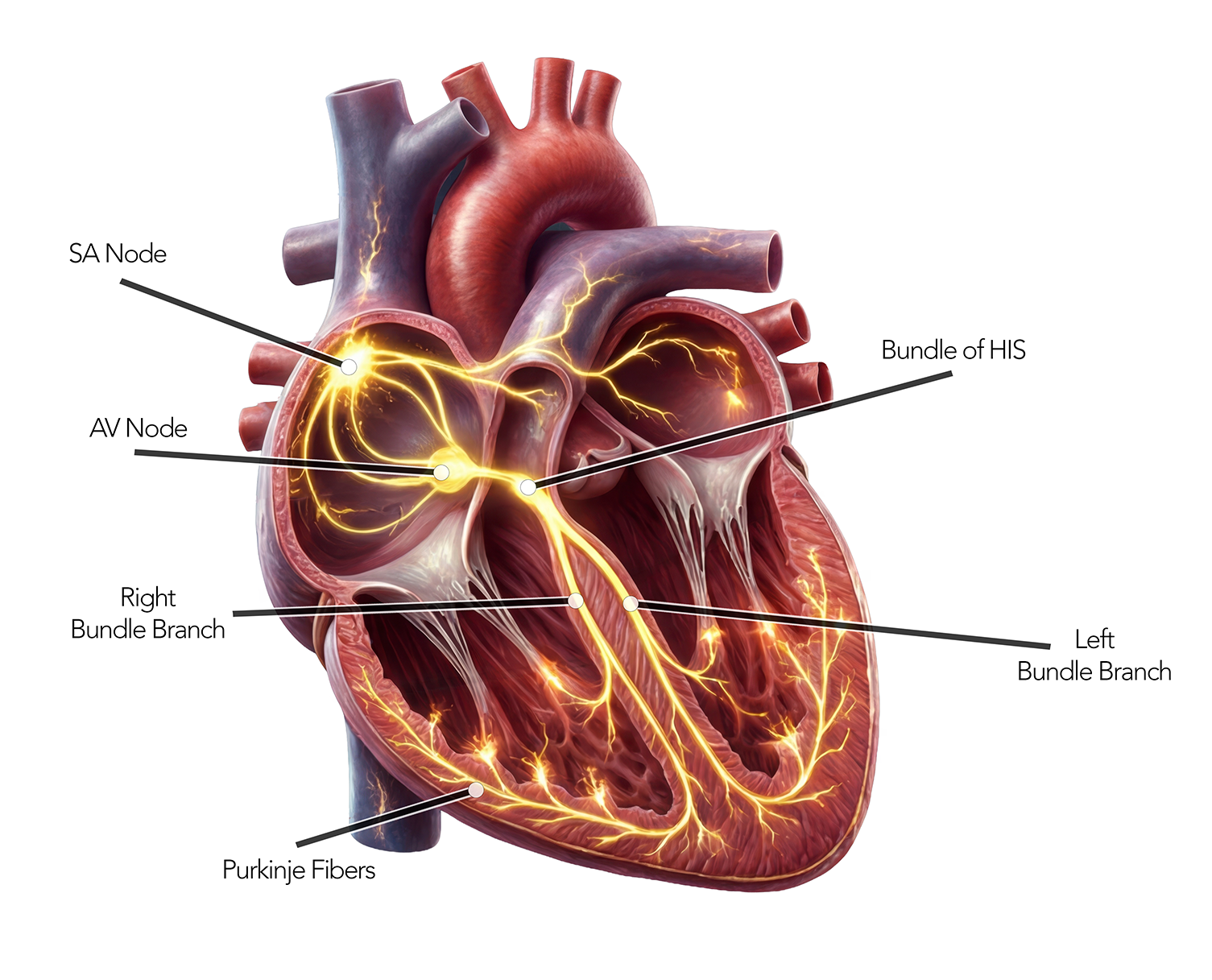
Every heartbeat starts as an electrical impulse, and the heart has its own built-in wiring to carry it. The signal follows the same path in the same order every time: it begins in the sinoatrial (SA) node in the right atrium and spreads across the atria, then pauses briefly at the AV node so the atria can finish emptying into the ventricles. From there it travels down the bundle of His, through the right and left bundle branches, and into the Purkinje fibers, which fire both ventricles almost at once. Because that sequence is so orderly, each step leaves its own fingerprint on the ECG, a distinct wave that appears in the same order on every beat.1
The SA node fires fastest, so it normally sets the pace, a rhythm we call "sinus rhythm." If it ever fails, slower backup pacemakers further down the pathway can step in to keep the heart beating.
- SA node: the pacemakerSpontaneously fires ~60–100×/min in the right atrium. Sets the heart rate.
- Atria depolarize → P waveThe impulse spreads across both atria, producing the P wave.
- AV node: the gatekeeperDeliberately delays the impulse (~0.1 s) so the atria can finish emptying. This pause is the flat PR segment.
- His bundle & bundle branchesThe signal speeds into the ventricular septum via the right and left bundle branches.
- Purkinje fibers → QRSFast fibers fire both ventricles almost simultaneously, the sharp QRS complex.
Anatomy of a heartbeat
Each part of the beat, what it is, and exactly where it sits on a real Lead II tracing. Colours match the Segment Lab; normal values follow the AHA/ACCF/HRS standardization series.134
P wave
Atrial depolarization
The electrical wave spreading across the right then left atrium, just before they squeeze. A small, smooth, rounded bump.
PR segment & interval
AV node delay
The flat line after the P wave is the AV node holding the impulse back so the atria can finish filling the ventricles. The PR interval spans the P wave start to the QRS start.
QRS complex
Ventricular depolarization
Both ventricles fire nearly together, driven by the fast Purkinje fibers, a tall, narrow spike. A Q is the first downward deflection, R the upward, S the downward after R.
J point
QRS–ST junction
The exact point where the QRS ends and the ST segment begins. It's the reference used to judge whether the ST segment is elevated or depressed.
ST segment
Plateau before recovery
The brief flat stretch when the ventricles are fully depolarized and holding, the action-potential "plateau." Normally level with the baseline; shifts here can signal injury.
T wave
Ventricular repolarization
The ventricles resetting electrically, ready for the next beat. A rounded, slightly asymmetric bump that normally points the same way as the QRS.
U wave
Late repolarization
A small, often invisible bump after the T wave, thought to reflect the last fibers (Purkinje / mid-myocardium) repolarizing. Prominent U waves can hint at low potassium.
QT interval
Total ventricular activity
Start of the QRS to the end of the T wave, the whole span of ventricular depolarization and recovery. It shortens as heart rate rises, so it's rate-corrected (QTc).
Reading the paper
ECG paper is standardised worldwide, so every box means the same thing. Time runs left-to-right; voltage runs up-and-down.1
Now read it yourself. Click two points on the strip to drop a caliper; it reads the span in seconds across and millivolts up. Count the boxes between your points to see where the numbers come from.
Finding the heart rate
On standard paper the gap between two R waves is the rate, count the large boxes between them and divide into 300.1 Tap a rate below to see exactly what it looks like on the grid.
Reading a rhythm, step by step
The same checklist works on every strip. Run it in order and the diagnosis usually names itself.
- Rate Fast, slow, or normal?
60–100 bpm is normal. < 60 = bradycardia, > 100 = tachycardia. - Regularity Are the R–R intervals even?
Regular, regularly-irregular, or irregularly-irregular (think AFib). - P waves What is the atrial activity?
Upright, uniform P = sinus origin. Sawtooth = flutter. Flat or fibrillatory = AFib or junctional. - PR interval Constant and 120–200 ms?
Applies only when P waves are present. Long or lengthening PR points to AV block. - P : QRS relationship Does every P conduct?
Dropped or dissociated beats reveal the type of block.
Now try it yourself. Work each strip through the checklist under the monitor; pick the finding that fits to move on, and the rhythm is named only at the end.
Common rhythms at a glance
The basics in action.67 Each card maps the rhythm back to the checklist above. See them live in the ecg_heartSimulator.
Normal sinus rhythm
60–100Regular · upright P before every QRS · PR 120–200 ms · narrow QRS.
The baseline. Everything else is judged against it.
Sinus bradycardia
< 60Same as sinus rhythm, just slow. Normal P–QRS–T, rate under 60.
Common in athletes and during sleep; can cause symptoms if too slow.
Sinus tachycardia
> 100Sinus rhythm sped up. Normal morphology, rate over 100, still regular.
Usually a response to something, fever, exercise, pain, dehydration.
Atrial fibrillation
irregularNo discrete P waves · wavy baseline · irregularly irregular R–R.
The atria quiver instead of contract, a major stroke-risk rhythm.
Atrial flutter
~150Sawtooth flutter waves (~300/min) · often regular at 2:1, 3:1 conduction.
A re-entry loop in the atrium; the ventricles follow at a fraction of the rate.
1° AV block
blockEvery P conducts, but the PR interval is long (> 200 ms) and fixed.
A slow gatekeeper, usually benign on its own.
2° AV block
blockMobitz I: PR lengthens until a QRS drops. Mobitz II: PR fixed, beats drop suddenly.
Mobitz II is the more dangerous: it can progress to complete block.
3° (complete) AV block
blockP waves and QRS march independently, no relationship between them.
The atria and ventricles are fully disconnected; an escape rhythm keeps things going.
You have the foundations: the waves, the grid, and a system to read them. Now see them in motion. Continue to Rhythm Foundations to study these common rhythms in depth and practice reading real-world ECGs.
Continue to Rhythm FoundationsReferences
Normal values and definitions follow the AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram series and related guidelines.
- Kligfield P, Gettes LS, Bailey JJ, et al. Recommendations for the standardization and interpretation of the electrocardiogram: Part I: The electrocardiogram and its technology. Circulation. 2007;115(10):1306–1324.
- Mason JW, Hancock EW, Gettes LS, et al. … Part II: Electrocardiography diagnostic statement list. Circulation. 2007;115(10):1325–1332.
- Surawicz B, Childers R, Deal BJ, et al. … Part III: Intraventricular conduction disturbances. Circulation. 2009;119(10):e235–e240.
- Rautaharju PM, Surawicz B, Gettes LS, et al. … Part IV: The ST segment, T and U waves, and the QT interval. Circulation. 2009;119(10):e241–e250.
- Wagner GS, Macfarlane P, Wellens H, et al. … Part VI: Acute ischemia/infarction. Circulation. 2009;119(10):e262–e270.
- Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay. Circulation. 2019;140(8):e382–e482.
- Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation. Circulation. 2024;149(1):e1–e156.
EKG Foundations is an educational reference for learning ECG interpretation. It is not medical advice and is not a substitute for clinical judgement or formal training.